Scientists at The Scripps Research Institute (TSRI) have devised a new antibiotic based on vancomycin that is powerfully effective against vancomycin-resistant strains of MRSA and other disease-causing bacteria.
The new vancomycin analog appears to have not one but two distinct mechanisms of anti-microbial action, against which bacteria probably cannot evolve resistance quickly.
“This is the prototype of analogues that once introduced will still be in clinical use a generation or maybe even two generations from now,” said Dale L. Boger, the Richard and Alice Cramer Professor of Chemistry at TSRI.
The report by Boger and members of his laboratory was published recently online ahead of print by the Journal of the American Chemical Society.
Increasing Reports of Resistance
Vancomycin entered clinical use in 1958, five years after its isolation from microbes in a soil sample gathered by an American missionary in Borneo. For nearly six decades it has been useful against a wide range of bacteria, and it remains a standard weapon against methicillin-resistant Staphylococcus aureus (MRSA), a major cause of hospital-acquired infections. A compound closely related to vancomycin also has been widely used to protect livestock.
Since the late 1980s, there have been increasing reports of vancomycin resistance in classes of bacteria that usually succumb to the antibiotic, including MRSA. Although vancomycin remains useful, scientists have been looking for new drugs to replace it in cases—often life-threatening—where it no longer can help patients.
The Boger laboratory has focused on inventing improved versions of vancomycin rather than entirely new compounds. “Vancomycin has lasted in clinical use for more than 50 years, in part because it isn’t very vulnerable to antibiotic resistance,” Boger said. “Our thought has been that if we find a vancomycin analog that addresses this current source of resistance we’ll get another 50 years of use out of it.”
Vancomycin works by binding to the building blocks of bacterial cell walls, in a way that prevents their proper assembly and leaves bacteria too leaky to live and replicate. The resistance comes from a single amino-acid alteration that some bacteria make to those building blocks, so that the antibiotic molecule can no longer get a firm grip. That drops vancomycin’s potency by a factor of about 1,000.
‘Incredibly Potent’
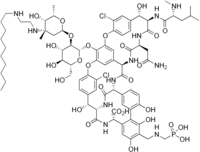
In 2012, Boger and his team reported making a vancomycin analog—informally termed vancomycin amidine—with a subtly altered binding pocket that fastens about equally well to the original and resistant sites on bacterial cell wall subunits. To get the precise structural modification they needed, they had to come up with a method for the “total synthesis” of this vancomycin-based compound—a controlled, step-by-step construction using organic chemistry reactions in the lab, rather than a natural enzyme-mediated production within cells.
“Years of work in this lab culminated in a total synthesis strategy that not only allowed us access to this target compound, but also gave us the ability to perform almost any other chemical modification of vancomycin that we wished,” said Akinori Okano, first author of the new report, who is an assistant professor of chemistry at TSRI.
Vancomycin amidine turned out to have acceptable level of activity against vancomycin-resistant and -sensitive bacteria, yet there was room for improvement. Thus in the new study, Okano, Boger and their colleagues used their vancomycin synthesis methods to add an additional feature to the molecule—a peripheral chlorobiphenyl (CBP), long known as a general booster of vancomycin’s potency.
“To our delight, the combination of these modifications led to an incredibly potent molecule, well beyond anything we had expected,” said Okano.